
BLOG

Tali AI Product Team
July 22, 2026


For primary care clinics across Ontario, managing a clinic day involves balancing patient care with a heavy volume of administrative tasks. Among these, clinical documentation and revenue tracking are two of the most time-consuming realities. Understanding how your EHR and medical billing processes interact is essential to keeping a clinic running efficiently. When documentation and financial workflows remain isolated from each other, family physicians face an increased administrative burden, lost hours, and preventable revenue leakage.
To build a better clinic workflow, it helps to look at the foundational EHR meaning in medical billing. The Electronic Health Record is the primary system of record where patient histories, clinical encounters, and lab reports are maintained. In the context of medical billing, the EHR acts as the legal and clinical justification for every single claim submitted to the Ministry of Health.
A billing claim cannot exist in a vacuum. Every code chosen must directly align with the documented details of the visit: the assessment, the diagnoses discussed, the complexity of the patient, and the exact time spent. This means that your billing workflow does not actually start on a billing screen or a separate portal. It begins the moment a family physician opens a chart and starts capturing an encounter.
When documentation and code selection are treated as completely separate tasks, clinicians are forced to rely heavily on memory or spend valuable time reconstructing past visits just to complete a submission page. This is why many clinics are now looking beyond basic billing tools and asking a bigger question: how well does our documentation workflow connect to billing?
In many clinics, documentation and billing still happen as separate tasks. The provider sees the patient, writes or dictates the note, completes the encounter, and then either remembers to add the right billing code or leaves part of the billing workflow to staff. If something is missing, someone has to go back into the chart, reconstruct the encounter, check the patient’s billing history, review eligibility rules, and decide what can be submitted.
That disconnect creates a few common problems:
For Ontario primary care, this is especially painful because OHIP billing is not just about choosing a code. It often requires understanding frequency limits, patient history, payment models, submission timing, rejection reports, and monthly reconciliation. Choosing an isolated medical billing software Ontario option or standalone OHIP billing software might help with typing out codes, but it fails to address the root issue: the data silo between clinical input and financial output.
Medical scribing and medical billing are often treated as completely separate categories, but in practice, they are closely connected. A scribe captures what happened in the encounter, while billing depends on what happened in the encounter. If the note is incomplete, inconsistent, or disconnected from the billing workflow, the claim becomes harder to support.
This is where AI medical billing and coding tools change the equation. Advanced workflows bring medical scribing and billing closer together by actively translating the clinical narrative into structural accuracy.
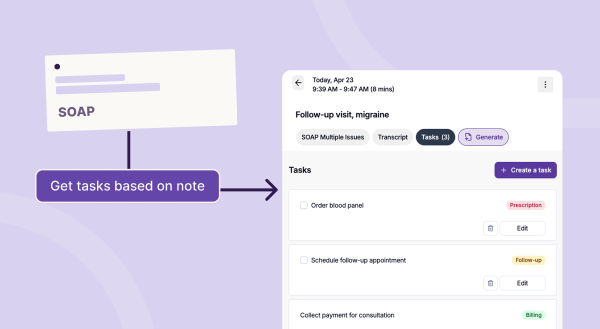
Instead of forcing the provider to finish documentation first and think about billing later, an AI-supported workflow brings these elements together:
Rather than forcing clinicians to act as data entry clerks, ambient technology transforms documentation into a launchpad for the entire billing cycle. To learn how an ambient entry point streamlines note-taking, explore the Tali AI Scribe features.

An integrated EHR and billing approach means the clinical workflow and billing workflow are connected, rather than handled as separate administrative steps. For providers, that means fewer manual handoffs. For clinics, it means billing can be supported by the exact context already captured in the note.
This integration is particularly critical for Ontario primary care clinics utilizing TELUS EMR platforms. If a billing tool sits outside the clinical workflow, providers must constantly copy, paste, remember, or manually verify information across multiple tabs and windows.
A unified workflow bridges these gaps directly within the platforms you already use every day:
By keeping these tools connected, clinics can eliminate duplicate entry and reduce the cognitive load that leads to documentation fatigue.
Ontario medical billing adds another layer of complexity because claims must move through rigid administrative cycles, strict submission timelines, and complex error-handling systems. For many clinics, the hard part is not only knowing which code to submit—it is managing everything that happens after the code is selected.
Ontario clinics must routinely manage:
This is why many Ontario providers describe billing as a second job. The work is not a single task—it is a chain of tasks, and each broken handoff creates more administrative burden downstream.
In Ontario, the MCEDT submission is the electronic pathway clinics use to exchange claims and reports with the Ministry. But submission is only the beginning. The real operational burden comes from what happens after submission: validating whether the file was accepted, reviewing error reports, correcting rejected claims, tracking timing against payment cycles, and reconciling what was eventually paid.
A billing workflow that only helps with submission does not solve the full problem. Rejected claims are not just cash flow delays—they create massive amounts of rework.
When a claim is rejected, someone has to investigate why. That often means going back to the original clinical note, checking patient details, reviewing the code, confirming eligibility, and deciding whether the claim can be corrected.
This is where disconnected workflows become expensive. If the clinical context is not structurally tied to the billing process, the person fixing the claim may need to reconstruct the patient visit from scratch. That takes time and increases the chance of another error. A better workflow reduces rework by helping providers and clinics catch billing issues earlier, while the encounter context is still fresh.
Even when claims are accepted, clinics still need to reconcile what was submitted against what was paid. The Remittance Advice report can include reduced payments, disallowed claims, explanatory codes, and other payment outcomes that require tedious manual interpretation. For clinic owners and providers, this is where billing becomes a financial visibility problem.
The clinic needs to understand:
Without a clean Remittance Advice reconciliation workflow, clinics cannot know whether billing issues are isolated mistakes or systemic errors. They may also completely miss short windows of opportunity to correct preventable revenue leakage.
For Ontario clinics evaluating how to optimize their administrative infrastructure, the key question is not simply: can this tool submit claims? A better question is: does this tool connect billing directly to the clinical workflow?
Look for a comprehensive strategy that supports your clinic from end to end:
| Workflow Stage | Operational Requirement |
|---|---|
| Documentation Context | The billing workflow must connect directly to the note, preventing providers from needing to recreate the visit hours later. |
| Billing Code Support | The system should help surface relevant diagnostic and billing codes based on the real-time encounter context. |
| Patient History Checks | For codes with strict frequency limits, the workflow should help verify eligibility rules early. |
| Error & Rejection Handling | The clinic needs clear, actionable insights into what went wrong with a claim and what needs to happen next to correct it. |
| RA Reconciliation | The system must make it easier to interpret monthly payment outcomes and identify missing or reduced revenue. |
Moving away from isolated software tools and toward a unified platform lets documentation naturally fuel financial operations, reducing manual effort across the clinical day.
For years, traditional software has focused entirely on the tail end of the administrative workflow: create the claim, submit it, fix errors, and reconcile payment. But the future of clinic operations is moving upstream. The most critical billing information is created during the encounter. If the clinical note, code selection, claim tracking, rejection workflow, and reconciliation process stay connected, billing ceases to be a reactive administrative chore.
That is the shift Ontario clinics need. Not more manual cleanup, disconnected reports, or a chaotic mess of tabs, portals, and spreadsheets. A better billing workflow starts directly in the EHR, follows the claim through submission and payment, and gives clinics absolute clarity into their operational health.
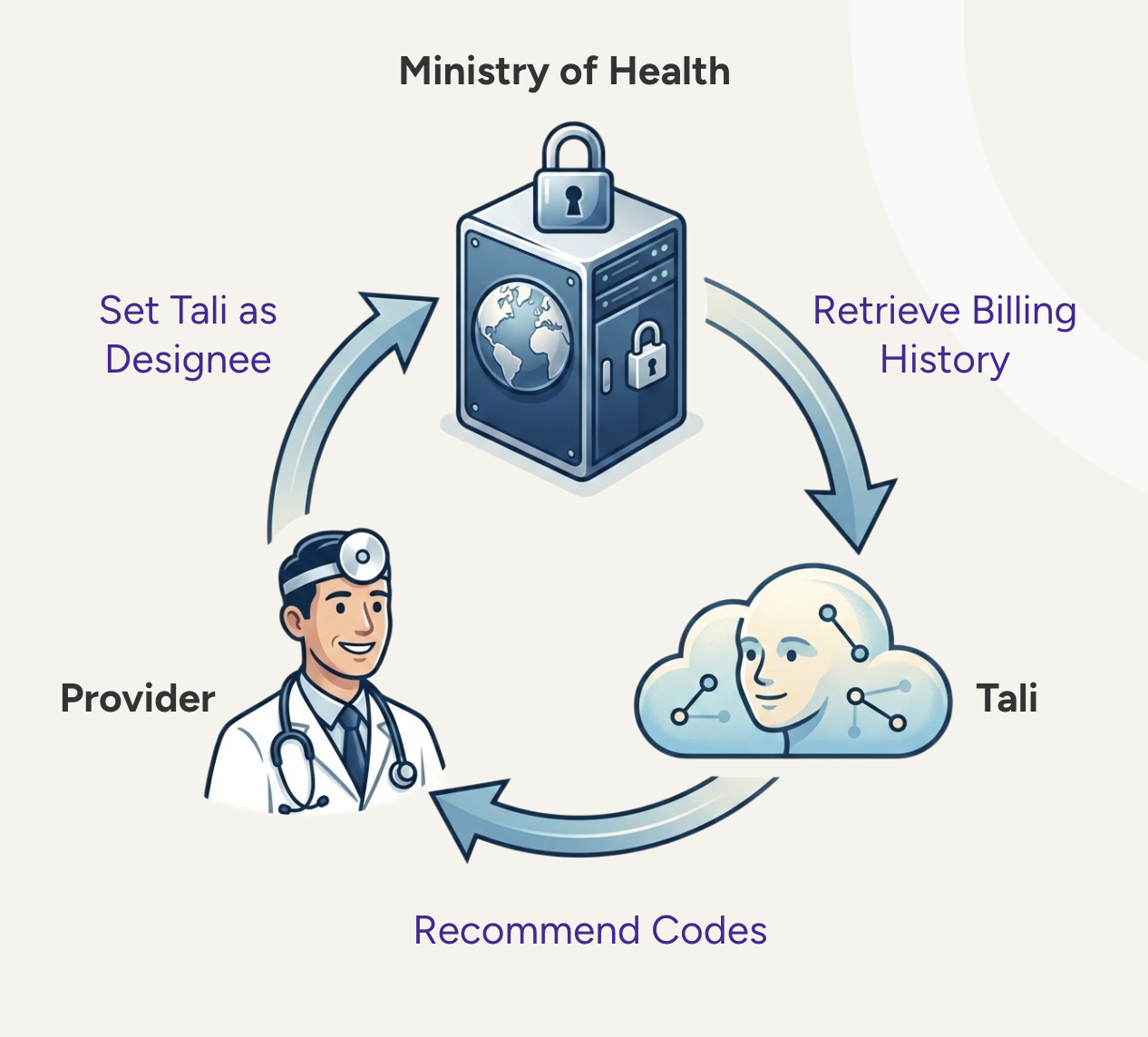
Tali is building billing workflows that smoothly connect clinical documentation, patient history, code recommendations, claim submission, and reconciliation. If your Ontario clinic is looking for a more intelligent way to manage OHIP billing, explore the Tali Realtime Billing Agent waitlist today.
EHR stands for Electronic Health Record. In medical billing, it refers to the digital clinical platform where encounters, assessments, and diagnostic details are stored. This documentation serves as the official clinical record needed to support and audit every billing claim submitted.
An integrated workflow connects clinical documentation directly to code selection and claim tracking. This eliminates duplicate data entry, reduces context switching for the provider, minimizes missed billing opportunities, and makes managing rejections much faster.
An AI scribe captures the natural conversation during a patient visit and structures it into a clinical note. Advanced workflow platforms can then analyze that structured context to suggest relevant diagnostic codes, helping Ontario family physicians verify that their documentation supports the intended OHIP codes before submission.
Remittance Advice reconciliation is the administrative process of matching the payment reports issued by the Ministry of Health against the original claims submitted by the clinic. This process helps teams identify which claims were fully paid, which were reduced, and which codes require correction and resubmission.
No. Integrated tools are designed to remove repetitive, manual data entry and provide better visibility into errors. They provide high-quality data and intelligent code suggestions, but final validation, submission management, and clinical accountability always remain with the healthcare team.
Experience the future of healthcare documentation with Tali's AI-powered solutions.
Start Free TrialRelated Articles
Clinician Burnout & Workflow
April 22, 2026

Clinician Burnout & Workflow
April 21, 2026

Clinician Burnout & Workflow
December 17, 2025

Research
July 22, 2026
12
Research
July 22, 2026
12
Research
July 22, 2026
12

